哌甲酯
| 本條目的引用需要进行清理,使其符合格式。 (2018年4月29日) |
body.skin-minerva .mw-parser-output table.infobox captiontext-align:center
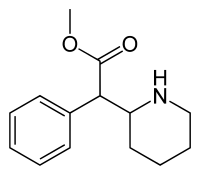 | |
 派醋甲酯 (Methylphenidate)的化學結構式 | |
| 系统(IUPAC)命名名称 | |
|---|---|
methyl 2-phenyl-2-(piperidin-2-yl)acetate | |
| 临床数据 | |
| 商品名 | Concerta, Methylin, Ritalin, Medikinet, Equasym XL, Quillivant XR, Metadate, Ritalin LA, Ritalin SR, Apo-Methylphenidate |
| Drugs.com | Monograph |
| MedlinePlus | a682188 |
| 医疗法规 |
|
| 妊娠分级 |
|
| 依赖性 | 生理: 无 心理: 中 |
| 成瘾性 | 中 |
| 给药途径 | 口服, 喷雾, 静脉, 经皮 |
| 合法狀態 | |
| 合法状态 |
|
药代动力学数据 | |
| 生物利用度 | ~30% (范围: 11–52%) |
| 蛋白结合度 | 10–33% |
| 代谢 | 肝脏 (80%) |
| 生物半衰期 | 2–3 小时[1] |
| 排泄 | 尿液 (90%) |
| 识别信息 | |
| CAS注册号 | 113-45-1 |
| ATC代码 | N06BA04 |
| PubChem | CID 4158 |
| IUPHAR/BPS | 7236 |
| DrugBank | DB00422 |
| ChemSpider | 4015 |
| UNII | 207ZZ9QZ49 |
| KEGG | D04999 |
| ChEBI | CHEBI:6887 |
| ChEMBL | CHEMBL796 |
| 其他名称 | 哌甲酯 、Methylphenidate |
| 化学信息 | |
| 化学式 | C14H19NO2 |
| 摩尔质量 | 233.31 g/mol |
SMILES
| |
InChI
| |
| 物理性质 | |
| 熔点 | 74 °C(165 °F) [2] |
| 沸点 | 136 °C(277 °F) [2] |
| (verify) | |
哌甲酯(英文:Methylphenidate),最常见的商品名为利他能(英语:Ritalin),是一种中樞神經系統興奮劑,被广泛应用于注意力缺陷多动障碍(ADHD)和嗜睡症的治疗。
哌甲酯的化學最簡式為C14H19NO2•HCl。 Methylphenidate hydrochloride USP 是一種白色、無味的結晶體。哌甲酯的水溶液介於酸性於鹼性之間。哌甲酯能在純水及甲醇中完全溶解;在乙醇中部分溶解;些微溶解於氯仿和丙酮中。Methylphenidate hydrochloride USP的分子量為269.77。[3]
哌甲酯在1948年由CIBA(后被诺华公司收购)研制,被用于治疗注意力缺陷多动障碍而在1955年获得FDA的销售许可,并在之后的几十年内成为医治该症的临床一线药物。[4]
哌甲酯用于医疗始于1960年。自20世纪90年代起,大眾逐漸接受ADHD的诊断,於是此药物的处方日益增加。在2007-2012年间,英国的哌甲酯处方增加了50%。[5][6]在2013年,全球的哌甲酯销售量增加到了24亿剂,与前一年同比上升66%。美国的消费量占全球的80%以上。 [7][8]
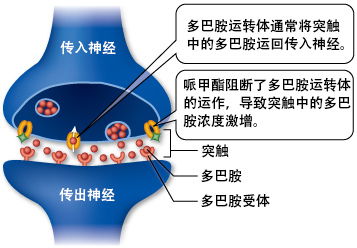
注意力缺陷多动障碍的病因可能与多巴胺、去甲肾上腺素和谷氨酸有关。这些物质决定了大脑的自我约束功能,并影响着人的注意力、控制力、行为、动机和执行能力。哌甲酯的作用便是抑制去甲肾上腺素和多巴胺的再摄取,使这些神经递质的浓度和强度大幅提高。哌甲酯和可卡因在结构和药理上有相似之处,但哌甲酯的效力低于后者,药效长于后者。[9][10][11][12][13]哌甲酯也是一种较弱的5HT1A受体兴奋剂。[14]
这一药品在全球范围内基本都受到不同程度的管制。
整體而言,哌甲酯與同為中樞神經興奮劑的安非他命結構上相似,但哌甲酯和安非他命不同,不容易造成成癮。用藥者應詳閱並遵照藥品說明書的指引。
目录
1 用途
1.1 医疗用途
1.1.1 注意力缺陷多动障碍
1.1.2 嗜睡症
1.1.3 其他
1.2 增强行为表现(益智藥)
1.2.1 增强行为表现的道德问题
2 禁忌症
3 药理學
3.1 药效学
3.2 药物代謝动力学
4 副作用
5 滥用
5.1 成瘾性与依赖性
5.1.1 生物分子机制
6 交互作用
6.1 v.s 阿托莫西汀
7 化学
7.1 体液中的检测
8 药物产品
8.1 利他能
8.1.1 藥品說明書(仿單)上的建議劑量
8.1.1.1 成人建議劑量
8.1.1.2 6-18歲的患者建議劑量
8.2 利長能
8.2.1 藥品說明書上的建議劑量
8.2.2 短效藥物轉換至長效利長能(Ritalin LA)的劑量轉換建議表
8.3 專思達
8.3.1 藥品說明書上的建議劑量
8.3.2 短效藥物轉換至長效專思達的劑量轉換建議表
8.4 安保美喜錠
8.5 維持療法
9 历史、社会与文化
9.1 法律状态
10 註解
11 延伸閱讀
11.1 參考資料
用途
医疗用途
哌甲酯是一种常见的兴奋剂类药物,药理是增加中枢神经系统的兴奋度。它所能产生的效果包括增加与保持警惕性、抵抗疲劳与提升注意力。哌甲酯的短期效益与成本效益已经确立。哌甲酯未被许可用于6岁以下的儿童。哌甲酯也可能用于治疗非适应症,例如躁郁症与重性抑郁障碍。
核磁共振的元分析与系统综述表明,长期使用ADHD兴奋剂(特别是安非他命与哌甲酯)可以减少ADHD受试者的大脑中的结构异常与功能异常。此外,临床兴奋剂研究的评论称已确定了长期连续使用ADHD兴奋剂对ADHD患者的安全性与有效性,长期所指的时间长达数年。然而,截至2015年11月,哌甲酯对患者的ADHD症状与生活质量的改善的精确度仍不明确。
注意力缺陷多动障碍
哌甲酯被美国食品与药品监督管理局(FDA)批准用于治疗注意力缺陷多动障碍。与行为修正与认知行为疗法配合治疗效果更佳。药物剂量的个体差异很大,因此使用的剂量必须精确。
ADHD当前的病理模型表明,ADHD与大脑中部分神经递质系统(尤其是涉及多巴胺与去甲肾上腺素的)中的功能障碍有关。哌甲酯与安非他命这一类的精神兴奋剂能够增加这些系统中的神经递质地活性,因而可能有效地治疗ADHD。约70%的使用者能改善ADHD的症状。使用哌甲酯的ADHD患儿通常能与同龄人与家庭成员建立更好的关系,在学校表现更好,且更少分心或冲动,能保持更久的注意力。ADHD患者的药物滥用失常可能性增加,而刺激性药物能降低这种风险。
嗜睡症
嗜睡症是一种慢性睡眠障碍,会导致在白天难以抑制的困倦,以及突然产生的困意,主要需要兴奋剂予以治疗。哌甲酯被认为有助于提升觉醒度、警惕性与行为表现。哌甲酯能改善标准化测试中嗜睡的结果,如多重睡眠潜伏期试验,但是不能提升到正常人的水平。
其他
哌甲酯也可能用于治疗重性抑郁障碍。它可以降低中风、癌症与HIV阳性患者的抑郁水平。然而,用兴奋剂治疗耐受性抑郁症的做法具有争议。在老人与病人身上,兴奋剂可能比三环类抗抑郁药具有更少的副作用。对于癌症晚期患者,哌甲酯可用于抵抗鸦片类药物导致的嗜睡,治疗抑郁症与改善认知功能。
增强行为表现(益智藥)
2015年,对高质量临床试验进行的荟萃分析与系统评价中发现,对于健康成人而言,治疗剂量的苯丙胺与哌甲酯可以造成认知能力(包括工作记忆、情景记忆和抑制控制试验)轻微但明确的改善,其作用机制为间接激活前额叶皮层的多巴胺受体D1与肾上腺皮质受体α2。哌甲酯与其他ADHD兴奋剂也可以提升任务的突出性与增强唤起。哌甲酯通过抑制再摄取中枢神经系统中的多巴胺来增加人的耐力与专注度。安非他命与哌甲酯这一类药物可以提升在执行枯燥与困难任务时的表现,并被某些学生用于学习与考试的辅助。基于自我报告的对兴奋剂违规使用的调查研究显示,提升表现而非用于娱乐,是学生使用兴奋剂的主要原因。与安非他命和安非他命酮类似,高于治疗剂量的哌甲酯可能对工作记忆与管控能力有负面影响,同时大剂量的哌甲酯还可能损害运动能力,如导致横纹肌溶解症与中暑。
增强行为表现的道德问题
哌甲酯有时被学生用来增强其精神能力,帮助集中注意力与帮助学习。
生物伦理学专家约翰·哈里斯认为,阻止健康人服用这种药物是不道德的。
他指出,如果人们可以接受一所大学“专门提升学生的精神能力,保证学生毕业时更加聪明,还能让它的学生比历史上任何学生都更聪敏”,并且为之高兴且都想把孩子送去的话,为什么在当下出现了这么一种“安全的、可以提升认知能力的药物”时,用药就成了不道德的呢?他提出阻止用药反而不道德。他声明称反对使用药物提升人类认知力是“不理性的”,且阻止了人类的发展。
Barbara Sahakian称这种使用利他林的方式可能导致学生在考试中拥有不公平的优势,最终导致大学可能会考虑要求学生提供尿样以进行药物检测。
禁忌症
以下情况禁用哌甲酯:
- 使用单胺氧化酶抑制剂(如苯乙肼、反苯环丙胺)时
- 有激越、抽动综合症、青光眼等情况
- 对哌甲酯药物中任何成分有超敏反应
美国FDA对哌甲酯的怀孕分级为C,建议女性只在效用超过潜在风险时使用。还没有足够的动物实验和人类研究足以说明哌甲酯对胎儿发育的作用。至2007年,实证文献中共包含来自3个实证研究的63条产前接触哌甲酯的案例。
药理學
药效学
Neurotransmitter transporter | Measure (units) | dl-MPH | d-MPH | l-MPH |
|---|---|---|---|---|
DAT | Ki (nM) | 121 | 161 | 2250 |
IC50 (nM) | 20 | 23 | 1600 | |
NET | Ki (nM) | 788 | 206 | >10000 |
| IC50 (nM) | 51 | 39 | 980 | |
SERT | Ki (nM) | >10000 | >10000 | >6700 |
| IC50 (nM) | — | >10000 | >10000 | |
GPCR | Measure (units) | dl-MPH | d-MPH | l-MPH |
5-HT1A | Ki (nM) | 5000 | 3400 | >10000 |
| IC50 (nM) | 10000 | 6800 | >10000 | |
5-HT2B | Ki (nM) | >10000 | 4700 | >10000 |
| IC50 (nM) | >10000 | 4900 | >10000 |
哌甲酯是一种苯哌啶衍生物。它与儿茶酚胺和苯乙胺有相同的基本结构。
哌甲酯主要充当去甲腎上腺素-多巴胺再攝取抑制劑(NDRI),一般有调整多巴胺水平在较小程度上也影响去甲肾上腺素的作用。[18] 与古柯碱相似,哌甲酯与多巴胺运转体(DAT)和去甲肾上腺素运转体(NET)结合并抑制其作用。[19]
此外,哌甲酯被认为是一种释放剂,通过提升多巴胺和去甲肾上腺素的释放,但作用不及安非他命。[20] 哌甲酯的作用机理被广泛争论,但和安非他命相比,它被认为加速了放电速率,而安非他命逆转了单胺运转体的流动。[21][22][23][24] 虽然两者作用都与多巴胺有关,但作用的方式明显不同。具体而言,哌甲酯是一种多巴胺再摄取抑制剂,而安非他命是一种促多巴胺释放剂。两者都对去甲肾上腺素有相应的微小作用。
哌甲酯具有多巴胺运转体和去甲肾上腺素运转体的亲和力,它的右旋对映体对去甲肾上腺素运转体显示了强烈的亲合势。左右两种对映体都显示了对5HT1A和5HT2B子类型的5-羟色胺受体的亲和力,尽管没有观察到和5-羟色胺转运体直接的结合。[17]
哌甲酯可能也会产生保护神经的作用。[25]
右旋对映体比左旋对映体效果甚佳[18],所以一些药物仅含有哌甲酯的右旋对映体。[來源請求]
药物代謝动力学
口服哌甲酯能达到11-52%的生物利用度,一次性释放(如利他林)其峰值效果能持续2-4小时,而缓释(如利他林SR)可持续3-8小时,或延长释放片剂可持续8-12小时(如Concerta)。哌甲酯的半衰期为2-3小时,取决于个体,服药约2小时后血浆浓度达到峰值。
口服给药时,哌甲酯的右旋同分异构体的生物利用度比其左旋同分异构体更高,且是哌甲酯外消旋混合物中起精神活性作用的主要物质。
与预计相反,在餐中服用哌甲酯可加快吸收。
哌甲酯在羧酸酯酶1的作用下代谢为利他林酸。右旋体与左旋体相比代谢速度更慢。
副作用
哌甲酯通常有高的耐受量。
观察到最常见的副作用包括食欲不振、口干、焦虑/紧张、恶心与失眠。
胃肠道的不良反应可包括腹部疼痛和体重减轻。
神经系统的副作用可包括坐立不安、易怒、运动障碍、困倦和头晕。
心脏的不良反应可包括心悸、血压变化、心率变化和心跳过速。
眼科方面的不良反应可能包括视力模糊和干眼,罕见复视与瞳孔扩大。
其他的副作用可能包括抑郁、情绪不稳、神志不清和磨牙。常见多汗,罕见胸痛。
有部分证据表明长期用药的儿童出现了略微的生长速度下降,但没有发现因果关系,且下降的情况没有长期存在。超敏反应(包括皮疹、荨麻疹和发烧)时有报道。
哌甲酯可以使精神病患者的精神病恶化,且在非常罕见的情况下可导致新的精神病症状的出现。由于此药物对狂躁与轻度狂躁有潜在的诱发性,在用于躁郁症患者时应特别小心。
有非常罕见的引发自杀念头的报道,但不足以建立因果联系。
偶尔有出血的报告。很少有导致性欲障碍、定向力障碍与幻觉的报道。阴茎异常勃起是其可能导致的非常罕见但可能严重的不良反应。
2011年,由FDA委托的研究表明,在儿童与成人中,哌甲酯或其他ADHD兴奋剂的医疗用途不会导致严重不良心血管事件(猝死,心脏病发作和中风)。
部分不良反应只在长期使用哌甲酯时出现,故应留意用药期间出现的不良反应。[26][27][28]
其他的副作用包括:[29]
- 腹痛
- 失静症 (烦躁不安)
- 脱发
- 暴躁
- 心绞痛
- 厌食症
- 焦虑
血压和脉搏变化 (上升和下降皆有可能)- 心律不整
- 憂鬱
- 出汗
- 眩晕
- 运动障碍
- 欣快或烦躁不安
- 头痛
过敏 (包括皮疹, 荨麻疹, 发热, 关节痛, 剥脱性皮炎, 多形性红斑, 坏死性脉管炎,和血小板减少性紫癜)- 倦怠
- 性欲变化
- 反胃
- 心悸
- 瞳孔放大[30]
- 精神失常[31]
- 暂时性体重减少
- 失眠
- 生长萎缩
- 自杀倾向
- 口腔干燥
滥用
哌甲酯急性过量的症状主要是因为中枢神经系统受到过度刺激。这些症状包括:呕吐、焦虑、震颤、反射亢进、肌肉抽搐、欣快、幻觉、谵妄、中暑、出汗、潮红、头痛、心跳过速、心律失常、心悸、高血压、瞳孔扩大和黏膜干燥。
严重的过量可能导致高热(不低于41.5℃)、肾上腺素过多、惊厥、偏执、刻板症、快速肌肉衰竭(横纹肌溶解症)、昏迷和循环衰竭。
有将哌甲酯片剂注射入动脉后导致脓肿和坏死的毒性反应的报道。
如果予以适当的救助,哌甲酯过量很少致命。
成瘾性与依赖性
药理学文章认为哌甲酯是一种效果、成瘾性、依赖性与苯丙胺(安非他命)类似的兴奋剂,而苯丙胺在可成瘾药物中处于中等。因此,当把哌甲酯高剂量使用作为娱乐性药物时,成瘾与心理依赖是可能的。当使用剂量大于医用剂量时,兴奋剂与兴奋剂型精神病的发展产生关联。与所有有成瘾性的药物一样,其成瘾机制为ΔFosB在伏隔核中的D1型中等有棘神经元中过量表达。
哌甲酯作为一种戒除甲基苯甲胺成瘾过程中的替代物质时表现出了一些好的效果。哌甲酯和安非他命已被研究作为可卡因成瘾治疗中的化学替代品,美沙酮也被以同样的方式用作替代药物治疗对海洛因的生理依赖。其在治疗可卡因或心理/生理成瘾方面的作用尚未证实,还有待进一步研究。
生物分子机制
因为哌甲酯在大脑的奖赏系统中的药物效应动力学作用(抑制多巴胺再摄取),其具有导致欣快的潜力。在治疗剂量下,ADHD兴奋剂不会充分激活奖赏系统,或者奖赏路径,以引起ΔFosB基因在伏隔核中的D1型中等有棘神经元中持久表达。因此,当用于医疗且遵照医嘱时,哌甲酯不会成瘾。然而,当哌甲酯以足够高的剂量通过高生物利用度的给药途径(如吸入或静脉注射)使用,尤其是用作兴奋剂时,ΔFosB会在伏隔核中积累。因此,与其他可成瘾药物一样,娱乐用途的高剂量哌甲酯最终会导致ΔFosB在伏隔核中的D1型中等有棘神经元中过量表达,随后引发一系列激活基因转录的信号转导,导致上瘾。
交互作用
哌甲酯可以抑制豆香素抗凝血剂、某些抗惊厥药物和一些抗抑郁药(三环类抗郁药和选择性5-羟色胺再摄取抑制剂)的代谢。共同给药可能需要调整剂量,可能需要监测血浆药物浓度来辅助。
[32]
有几例哌甲酯与抗郁药共同使用诱发血清素综合征的案例。
[33][34]
与酒精的混合作用可导致d-哌甲酯的血浆浓度上升最多40%。
[35]
哌甲酯的肝毒性极其罕见,但有限的证据表明,与哌甲酯共同摄入β肾上腺素激动剂可能增加肝中毒的风险。
[36]
v.s 阿托莫西汀
阿托莫西汀為另一種常見用於治療注意力不足/過動症(AD/HD)的第一線藥物。
縱然阿托莫西汀與中樞神經興奮劑同樣為治療ADHD的第一線藥物,然而其對特定症狀改善的程度可能與中樞神經興奮劑不同(兩類藥物各有其長處)。阿托莫西汀在改善過動-衝動的症狀上,略優於派甲酯;派甲酯則在改善分心的症狀上,略優於阿托莫西汀。[37][38][39]
而阿托莫西汀與哌甲酯併服的處方尚未經美國食品藥物管理局核可,但醫師會視個案的情況(如共病、預後)以開仿單標示外使用的方式處方之。[40][41][42][43]在臨床試驗中,並未發現兩者併服後產生加乘的心血管副作用。換言之,兩者併服之心血管副作用,與單獨服用哌甲酯所產生的心血管副作用相同。[44]
化学
哌甲酯可能有四种同分异构体,因为其分子具有两个手性中心,可分为一对赤式与一对苏式异构体,其中只有右-苏式-哌甲酯有药物活性。当此药刚上市时,以赤式:苏式按3:1混合。赤式非对映异构体也是升压胺。
体液中的检测
哌甲酯及其主要代谢物利他林酸可在血浆、血清或全血中检验,以监测病人是否按医嘱用药,确认可能的中毒者,或协助剂量致命时的法医调查。
药物产品
以下藥品所含之有效成分皆為哌甲酯,各自在藥效動力學上具有相同屬性;在藥物代謝動力學上的作用則有些微差異。
- 利他能(Ritalin)[45]
- 利長能(Ritalin LA)[46]
- 專思達(Concerta)[47]
- 安保美喜錠(Apo-Methylphenidate)[48][49]
藥品的劑量應採個人化的方式視患者的反應及需要來決定之。[50]
利他能
有5、 10、 和 20 mg 等三種口服錠劑型。[51]
作用時間:約3.5小時。
藥品說明書(仿單)上的建議劑量
成人建議劑量
多數患者的平均劑量為每天總劑量20-30毫克(mg),並在一天中分2-3次達成。建議在餐前30-45分鐘前服用。有些患者的每日總劑量可能需要到達40-60毫克,並在一天中分2-3次達成。除了以上兩者,患者的每日總劑量約控制在10-15 毫克,並在一天中分2-3次達成即可。
[52]
6-18歲的患者建議劑量
起始劑量為分別在早餐和午餐前服用一顆5毫克的利他能。並視需要,以一個星期為一次劑量的調整週期,每次調整的幅度為5或10毫克(mg)。無論分幾次服用,每天的總劑量不建議超過60毫克。
[53]
利長能
利長能共有 10、 20、 30、 40和 60 毫克五種劑型,分別與每日服用兩次的短效利他能之5、 10、 15、 20、 和 30 毫克(mg)劑型相對應。[54]
藥品說明書上的建議劑量
建議起始劑量為每天一粒20毫克的利長能。然而醫師可依照臨床判斷將起始劑量降至每天一粒 10毫克的利長能。往後的日子中,劑量的調整建議以一周調整10毫克(mg)為準。利長能的劑量可依照患者對藥物的耐受性及症狀改善的程度將劑量以一周調整10毫克的準則,逐漸調整至每天一粒60毫克的利長能。然而不建議將劑量繼續增加到超過60毫克/每天。
[55]
藥效作用時間:約8小時。
短效藥物轉換至長效利長能(Ritalin LA)的劑量轉換建議表
| (Previous Methylphenidate Dose) | (Recommended Ritalin LA Dose) |
|---|---|
| 每天服用5毫克的利他能二次 | 每天一粒10毫克的利長能 (10 mg q.d.) |
| 每天服用10毫克的利他能二次或20mg的methylphenidate-SR | 每天一粒20毫克的利長能(20 mg q.d.) |
| 每天服用15毫克的利他能二次 | 每天一粒30毫克的利長能 (30 mg q.d.) |
| 每天服用20毫克的利他能二次或40mg的methylphenidate-SR | 每天一粒40毫克的利長能(40 mg q.d.) |
| 每天服用30毫克的利他能二次或60mg的methylphenidate-SR | 每天一粒60毫克的利長能(60 mg q.d.) |
[56]
專思達
藥效持續時間:約十二小時。
[57]
藥品說明書上的建議劑量
| 患者年紀 | 建議起始劑量 | 劑量範圍 |
|---|---|---|
| 6-12歲 | 18 毫克/每天 | 18 - 54 毫克/每天 |
| 13-17歲 | 18 毫克/每天 | 18 - 72 毫克/每天 每天每公斤不可超過2毫克。[註 1] |
| 18-65歲 | 18 毫克/每天 | 18 - 72 毫克/每天 |
[47]
註解:
- 在專思達的藥物試驗過程中發現,13-17歲的青年試驗組中,專思達的最低有效劑量為: 每天每公斤1.4毫克。[58]
- 18歲以上的兩個成人試驗組中,發現每天18-72毫克的劑量皆可達到在統計學上具顯著意義的療效,然而以每天36毫克以上進而達到統計學上具顯著意義的療效的臨床試驗者為大多數。
[59]
短效藥物轉換至長效專思達的劑量轉換建議表
| 短效利他能的每天總劑量 | 建議轉換至專思達的劑量 |
|---|---|
| 每天服用5毫克的利他能二至三次 | 每天早上服用一顆18毫克的專思達 |
| 每天服用10毫克的利他能二至三次 | 每天早上服用一顆36毫克的專思達 |
| 每天服用15毫克的利他能二至三次 | 每天早上服用一顆54毫克的專思達 |
| 每天服用20毫克的利他能二至三次 | 每天早上服用一顆72毫克的專思達 |
[47]
註解:
- 台灣尚未引進72毫克之專思達。
安保美喜錠
安保美喜錠(Apo-Methylphenidate)為利他能的副廠藥品。 副廠名:Apotex Incorporation. [48]
維持療法
患者所需的藥物治療時間因人而異。然而學界普遍認為,藥物治療通常不能太短。患者與醫師應該定期追蹤自己以及患者的病況。患者的症狀有可能在暫時或永久停藥後繼續改善,倘若如此,則可能是停藥時機點。
[60]
历史、社会与文化
法律状态
- 在全球范围内,哌甲酯是《精神药物公约》中的Schedule II类药物。
- 在美国,哌甲酯被分类为Schedule II管制物质,即有公认的医疗价值但具有高的滥用可能性。
- 在英国,哌甲酯是B类受管制物质。无处方而持有哌甲酯可处以最高五年有期徒刑和/或无上限的罚款,非法售卖可处以最高14年有期徒刑和/或无上限的罚款。
- 在加拿大,哌甲酯被列入《管制药物与物质法》中的Schedule III(与LSD、迷幻蘑菇、酶斯卡灵等同一分类),且无处方持有哌甲酯为非法。
- 在新西兰,哌甲酯是B2类管制物质,非法持有可处以六个月有期徒刑,非法出售可处以14年有期徒刑。
- 在澳大利亚,哌甲酯是Schedule 8管制物质。此类物质在出售前必须放置在可上锁的保险箱内,无处方持有可被处以巨额罚款甚至监禁。
- 在瑞典,哌甲酯是List II类管制物质,具有公认的医疗价值。无处方持有可被处以最高三年的有期徒刑。
- 在法国,哌甲酯被分类为麻醉剂,开处方与售卖被严格管制,只能在开出处方的医院购买(hospital-only prescription),用于初次治疗以及每年一度的咨询。
- 在印度,哌甲酯是Schedule X药物且受1945年发布的《药物与化妆品法案》管制,只能凭神经病专家或精神科医生开出的处方购买。
- 在台湾,哌甲酯依例为第三级管制药品,医师处方需使用管制药品专用处方笺。[61]
- 在中华人民共和国,这一药物属于第一类精神药品,[62]管制措施与其他精神兴奋剂(如苯丙胺和莫达非尼)相同。不过不同于其他第一类精神药品和麻醉药品的是,哌甲酯控缓释制剂用于治疗儿童注意缺陷多动障碍,可一次处方15日量(而非一般精麻药品控缓释制剂的7日量)。[63]
註解
^ 舉例:一個三十公斤的服藥者每天不可服用超過60毫克的專思達
延伸閱讀
- 注意力不足過動症
- 嗜睡症
參考資料
^ Kimko, HC; Cross, JT; Abernethy, DR. Pharmacokinetics and clinical effectiveness of methylphenidate.. Clinical pharmacokinetics. December 1999, 37 (6): 457–70. PMID 10628897. doi:10.2165/00003088-199937060-00002.
^ 2.02.1 Chemical and Physical Properties. Methylphenidate. Pubchem Compound. National Center for Biotechnology Information. [24 June 2014].
^ Label of Ritalin. DailyMed. Novartis. January 5, 2017 [March, 2017.].Methylphenidate hydrochloride USP is a white, odorless, fine crystalline powder. Its solutions are acid to litmus. It is freely soluble in water and in methanol, soluble in alcohol, and slightly soluble in chloroform and in acetone. Its molecular weight is 269.77.
请检查|access-date=中的日期值 (帮助)
^ www.ehow.com/about_5374709_ritalin-invented.html When Was Ritalin Invented?, citing Lawrence Diller: "Running on Ritalin", 1999
^
Diller, Lawrence. Running on Ritalin. 1999. ISBN 978-0553379068.
^
Lange KW, Reichl S, Lange KM, Tucha L, Tucha O. The history of attention deficit hyperactivity disorder. ADHD Attention Deficit and Hyperactivity Disorders. 2010, 2 (4): 241–55. PMC 3000907. PMID 21258430. doi:10.1007/s12402-010-0045-8.
^ ADHD drug use 'up 50% in six years'. 2013-08-13 –通过www.bbc.com.
^ Narcotics monitoring board reports 66% increase in global consumption of methylphenidate.
^ "Ritalin & Cocaine: The Connection and the Controversy". Learn.genetics.utah.edu. Retrieved on 2011-10-16.
^
Mary Ann Boyd. Psychiatric nursing: contemporary practice. Lippincott Williams & Wilkins. 2005: 160– [30 April 2011]. ISBN 978-0-7817-4916-9.
^
Peter Doskoch. Why isn't methylphenidate more addictive?. NeuroPsychiatry Rev. 2002, 3 (1): 19. (原始内容存档于2009-03-30).
^
Functional Roles of Norepinephrine and Dopamine in ADHD: Dopamine in ADHD. Medscape. 2006 [8 October 2013].Catecholamines not only facilitate attention, they are essential to executive function. The prefrontal cortex directs behaviors, thoughts, and feelings represented in working memory. This representational knowledge is essential to fundamental cognitive abilities that compromise executive functions. These encompass the ability to (1) inhibit inappropriate behaviors and thoughts, (2) regulate our attention, (3) monitor our actions, and (4) plan and organize for the future. Difficulties with these prefrontal cortex functions are evident in neuropsychological and imaging studies of ADHD patients and account for many of the common behavioral symptoms. Measures of prefrontal cortical functioning in animals indicate that these functions are sensitive to small changes in catecholamine modulation of prefrontal cortex cells that can produce profound effects on the ability of the prefrontal cortex to guide behavior. Optimal levels of NE acting at postsynaptic alpha2A-adrenoceptors and dopamine acting at D1 receptors are essential to prefrontal cortex function. Blockade of norepinephrine alpha2-adrenoceptors in prefrontal cortex markedly impairs prefrontal cortex function and mimics most of the symptoms of ADHD, including impulsivity and locomotor hyperactivity. Conversely, stimulation of prefrontal cortical alpha2-adrenoceptors strengthens prefrontal cortex regulation of behavior and reduces distractibility. Thus, effective treatments for ADHD facilitate catecholamine transmission and apparently have their therapeutic actions by optimizing catecholamine actions in the prefrontal cortex
^
Arnsten AF, Li BM. Neurobiology of Executive Functions: Catecholamine Influences on Prefrontal Cortical Functions. Biological Psychiatry. 2005, 57 (11): 1377–84. PMID 15950011. doi:10.1016/j.biopsych.2004.08.019.
^
Markowitz JS, DeVane CL, Ramamoorthy S, Zhu HJ. The psychostimulant d-threo-(R,R)-methylphenidate binds as an agonist to the 5HT(1A) receptor.. Pharmazie. Feb 2009, 64: 123–5. PMID 19322953.
^ Markowitz, JS; Patrick, KS. Differential pharmacokinetics and pharmacodynamics of methylphenidate enantiomers: does chirality matter?. Journal of Clinical Psychopharmacology. June 2008, 28 (3 Suppl 2): S54–61. PMID 18480678. doi:10.1097/JCP.0b013e3181733560.
^ Williard, RL; Middaugh, LD; Zhu, HJ; Patrick, KS. Methylphenidate and its ethanol transesterification metabolite ethylphenidate: brain disposition, monoamine transporters and motor activity.. Behavioural Pharmacology. February 2007, 18 (1): 39–51. PMID 17218796. doi:10.1097/fbp.0b013e3280143226.
^ 17.017.1 Markowitz, JS; DeVane, CL; Pestreich, LK; Patrick, KS; Muniz, R. A comprehensive in vitro screening of d-, l-, and dl-threo-methylphenidate: an exploratory study.. Journal of child and adolescent psychopharmacology. December 2006, 16 (6): 687–98. PMID 17201613. doi:10.1089/cap.2006.16.687. 引用错误:带有name属性“pmid17201613”的<ref>标签用不同内容定义了多次
^ 18.018.1 Heal DJ, Pierce DM. Methylphenidate and its isomers: their role in the treatment of attention-deficit hyperactivity disorder using a transdermal delivery system. CNS Drugs. 2006, 20 (9): 713–38. PMID 16953648. doi:10.2165/00023210-200620090-00002.
^ Iversen L. Neurotransmitter transporters and their impact on the development of psychopharmacology. British Journal of Pharmacology. 2006, 147 (Suppl 1): S82–8. PMC 1760736. PMID 16402124. doi:10.1038/sj.bjp.0706428.
^ Sulzer D, Sonders MS, Poulsen NW, Galli A. Mechanisms of neurotransmitter release by amphetamines: a review (PDF). Prog. Neurobiol. 2005, 75 (6): 406–33. PMID 15955613. doi:10.1016/j.pneurobio.2005.04.003.
^ Viggiano D, Vallone D, Sadile A. Dysfunctions in dopamine systems and ADHD: evidence from animals and modeling. Neural Plasticity. 2004, 11 (1–2): 102, 106–107. PMC 2565441. PMID 15303308. doi:10.1155/NP.2004.97. Full-text [1]
^ Novartis: Focalin XR Overview
^ Focalin XR – Full Prescribing Information. Novartis.
^ SPC Concerta XL 18 mg – 36 mg prolonged release tablets last updated on the eMC: 05/11/2010
^ T. J. Volz. Neuropharmacological Mechanisms Underlying the Neuroprotective Effects of Methylphenidate. Current Neuropharmacology. 2008. PMC 2701286. doi:10.2174/157015908787386041.
^ Gordon N. Attention deficit hyperactivity disorder: possible causes and treatment. Int. J. Clin. Pract. 1999, 53 (7): 524–8. PMID 10692738.
^ King S, Griffin S, Hodges Z; 等. A systematic review and economic model of the effectiveness and cost-effectiveness of methylphenidate, dexamfetamine and atomoxetine for the treatment of attention deficit hyperactivity disorder in children and adolescents. Health Technol Assess. 2006, 10 (23): iii–iv, xiii–146. PMID 16796929. 引文格式1维护:显式使用等标签 (link)
^ Gonzalez de Dios J, Cardó E, Servera M. [Methylphenidate in the treatment of attention-deficit/hyperactivity disorder: are we achieving an adequate clinical practice?]. Rev Neurol. 2006, 43 (12): 705–14. PMID 17160919 (Spanish; Castilian). 引文格式1维护:未识别语文类型 (link)
^ – Ritalin Side Effects. Drugs.com. Retrieved on 2011-10-16.
^ Jaanus SD. Ocular side-effects of selected systemic drugs. Optom Clin. 1992, 2 (4): 73–96. PMID 1363080.
^ Auger RR, Goodman SH, Silber MH, Krahn LE, Pankratz VS, Slocumb NL. Risks of high-dose stimulants in the treatment of disorders of excessive somnolence: a case-control study. Sleep. 2005, 28 (6): 667–72. PMID 16477952.
^
Concerta product monograph (PDF). Janssen Pharmaceuticals. [4 December 2016].
^
Markowitz JS, Logan BK, Diamond F, Patrick KS. Detection of the novel metabolite ethylphenidate after methylphenidate overdose with alcohol coingestion. Journal of Clinical Psychopharmacology. 1999, 19 (4): 362–6. PMID 10440465. doi:10.1097/00004714-199908000-00013.
^
Markowitz JS, DeVane CL, Boulton DW, Nahas Z, Risch SC, Diamond F, Patrick KS. Ethylphenidate formation in human subjects after the administration of a single dose of methylphenidate and ethanol. Drug metabolism and disposition: the biological fate of chemicals. 2000, 28 (6): 620–4. PMID 10820132.
^
Patrick KS, Straughn AB, Minhinnett RR, Yeatts SD, Herrin AE, DeVane CL, Malcolm R, Janis GC, Markowitz JS. Influence of ethanol and gender on methylphenidate pharmacokinetics and pharmacodynamics.. Clinical pharmacology and therapeutics. March 2007, 81 (3): 346–53. PMC 3188424. PMID 17339864. doi:10.1038/sj.clpt.6100082.
^
Roberts SM, DeMott RP, James RC. Adrenergic modulation of hepatotoxicity. Drug Metab. Rev. 1997, 29 (1–2): 329–53. PMID 9187524. doi:10.3109/03602539709037587.
^ Chi-Yung Shang, Yi-Lei Pan, Hsiang-Yuan Lin, Lin-Wan Huang & Susan Shur-Fen Gau. An Open-Label, Randomized Trial of Methylphenidate and Atomoxetine Treatment in Children with Attention-Deficit/Hyperactivity Disorder. Journal of child and adolescent psychopharmacology. September 2015, 25 (7): 566–573. PMID 26222447. doi:10.1089/cap.2015.0035.At week 24, mean changes in ADHD-RS-IV Inattention scores were 13.58 points (Cohen's d, -3.08) for OROS-methylphenidate and 12.65 points (Cohen's d, -3.05) for atomoxetine; and mean changes in ADHD-RS-IV Hyperactivity-Impulsivity scores were 10.16 points (Cohen's d, -1.75) for OROS-methylphenidate and 10.68 points (Cohen's d, -1.87) for atomoxetine.
^ 中華民國衛生福利部/心理衛生專輯/03注意力不足過動症.pdf (PDF). http://www.mohw.gov.tw/. 中華民國衛生福利部. June 2015 [February 2017]. (原始内容 (PDF)存档于June 2015).一般發現其對於專注度的改善沒有 MPH 明顯
^ 3, 注意力不足過動症 (PDF), 中華民國衛生福利部/心理衛生專輯 1 1, 中華民國衛生福利部/心理衛生專輯/03注意力不足過動症.pdf: 中華民國衛生福利部: 22, [June 2015], ISBN 9789860454154, (原始内容 (PDF)存档于June 2015) (Chinese Traditional及繁體中文),atomoxetine,用在病情 較為複雜、或是無法忍受MPH副作用的患者,然而一般發現其對於專注度的改善沒有MPH明顯
引文格式1维护:未识别语文类型 (link)
^ Parent's Medication Guide: ADHD (PDF). American Psychiatric Association (Guidelines (Tertiary source)). American Psychiatric Association & American Academy of Child and Adolescent Psychiatry (AACAP). July 2013 [January 2017]. (原始内容存档于July 2013).Though not FDA-approved for combined treatment, atomoxetine (Strattera) is sometimes used in conjunction with stimulants as an off-label combination therapy.
^ Medical Encyclopedia → Attention deficit hyperactivity disorder. MedlinePlus.gov. 2017-01-05 [January 2017].Medicine combined with behavioral treatment often works best. Different ADHD medicines can be used alone or combined with each other. The doctor will decide which medicine is right, based on the person's symptoms and needs.
^ Treuer T, Gau SS, Méndez L, Montgomery W, Monk JA, Altin M; 等. A systematic review of combination therapy with stimulants and atomoxetine for attention-deficit/hyperactivity disorder, including patient characteristics, treatment strategies, effectiveness, and tolerability.. Journal of Child and Adolescent Psychopharmacology (systematic review (Secondary source)). 2013, 23 (3): 179–93. PMC 3696926. PMID 23560600. doi:10.1089/cap.2012.0093.Existing evidence suggests, but does not confirm, that this drug combination may benefit some, but not all, patients who have tried several ADHD medications without success.
引文格式1维护:显式使用等标签 (link)
^ Perugi G, Vannucchi G. The use of stimulants and atomoxetine in adults with comorbid ADHD and bipolar disorder.. Expert Opin Pharmacother. 2015, 16 (14): 2193–204. PMID 26364896. doi:10.1517/14656566.2015.1079620.Although systematic trials on the use of stimulants and ATX in ADHD-BD comorbidity in adulthood are necessary, both treatments should be considered possible options to be carefully evaluated once the patient has been stabilized.
^ Label of Strattera consisting of atomoxetine. DailyMed.gov (Leaflet/label (Tertiary source)). Eli Lilly Company. June 2015 [February 2017].7.7 Methylphenidate Coadministration of methylphenidate with STRATTERA did not increase cardiovascular effects beyond those seen with methylphenidate alone.
^ Label of Ritalin. DailyMed. Novartis. January 5, 2017 [March, 2017.]. 请检查|access-date=中的日期值 (帮助)
^ Label of Ritalin LA (PDF). Novartis.com. Novartis. Mid 2015 [January, 2017.]. 请检查|access-date=, |date=中的日期值 (帮助)
^ 47.047.147.2
Label of Concerta (PDF). concerta.net. Jassen Cilag. 2013 [January, 2017.]. 请检查|access-date=中的日期值 (帮助)
^ 48.048.1
Apotex Incorporation., 安保美喜錠 10 毫克 衛署藥輸字第 025016 號, (编) 鴻汶醫藥實業有限公司, Information for the patient (PDF), Canada, March 27, 2006 [2017-03-19]
^
安保美喜錠 10 毫克 衛署藥輸字第 025016 號 (PDF), Canada: Apotex Incorporation., March 27, 2006 [2017-03-19]
^
Label of Ritalin LA. DailyMed.com. Novartis. Mid 2015 [January, 2017.].Dosing Recommendations:Dosage should be individualized according to the needs and responses of the patients.)
请检查|access-date=, |date=中的日期值 (帮助)
^ Label of Ritalin. DailyMed. Novartis. January 5, 2017 [March, 2017.].Ritalin hydrochloride, methylphenidate hydrochloride USP, is a mild central nervous system (CNS) stimulant, available as tablets of 5, 10, and 20 mg for oral administration;
请检查|access-date=中的日期值 (帮助)
^
Label of Ritalin. DailyMed.com. Novartis. January 5, 2017 [March, 2017.].Dosage should be individualized according to the needs and responses of the patient.
参数
Adults
Tablets: Administer in divided doses 2 or 3 times daily, preferably 30 to 45 minutes before meals. Average dosage is 20 to 30 mg daily. Some patients may require 40 to 60 mg daily. In others, 10 to 15 mg daily will be adequate. Patients who are unable to sleep if medication is taken late in the day should take the last dose before 6 p.m.
SR Tablets: Ritalin-SR tablets have a duration of action of approximately 8 hours. Therefore, Ritalin-SR tablets may be used in place of Ritalin tablets when the 8-hour dosage of Ritalin-SR corresponds to the titrated 8-hour dosage of Ritalin. Ritalin-SR tablets must be swallowed whole and never crushed or chewed.|quote=值左起第85位存在換行符 (帮助); 请检查|access-date=中的日期值 (帮助)
^
Label of Ritalin. DailyMed.com. Novartis. January 5, 2017 [March, 2017.].Dosage should be individualized according to the needs and responses of the patient.
参数
Children (6 years and over)
Ritalin should be initiated in small doses, with gradual weekly increments. Daily dosage above 60 mg is not recommended.
If improvement is not observed after appropriate dosage adjustment over a 1-month period, the drug should be discontinued.
Tablets: Start with 5 mg twice daily (before breakfast and lunch) with gradual increments of 5 to 10 mg weekly.
SR Tablets: Ritalin-SR tablets have a duration of action of approximately 8 hours. Therefore, Ritalin-SR tablets may be used in place of Ritalin tablets when the 8-hour dosage of Ritalin-SR corresponds to the titrated 8-hour dosage of Ritalin. Ritalin-SR tablets must be swallowed whole and never crushed or chewed.|quote=值左起第85位存在換行符 (帮助); 请检查|access-date=中的日期值 (帮助)
^
Label of Ritalin LA. DailyMed.com. Novartis. Mid 2015 [January, 2017.].Methylphenidate hydrochloride is a central nervous system (CNS) stimulant.
参数
Ritalin LA® (methylphenidate hydrochloride) extended-release capsules is an extended-release formulation of methylphenidate with a bi-modal release profile. Ritalin LA uses the proprietary SODAS® (Spheroidal Oral Drug Absorption System) technology. Each bead-filled Ritalin LA capsule contains half the dose as immediate-release beads and half as enteric-coated, delayed-release beads, thus providing an immediate release of methylphenidate and a second delayed release of methylphenidate. Ritalin LA 10, 20, 30, 40, and 60 mg capsules provide in a single dose the same amount of methylphenidate as dosages of 5, 10, 15, 20, or 30 mg of Ritalin tablets given b.i.d.)|quote=值左起第75位存在換行符 (帮助); 请检查|access-date=, |date=中的日期值 (帮助)
^
Label of Ritalin LA. DailyMed.com. Novartis. Mid 2015 [January, 2017.].Initial Treatment
参数
The recommended starting dose of Ritalin LA is 20 mg once daily. Dosage may be adjusted in weekly 10 mg increments to a maximum of 60 mg/day taken once daily in the morning, depending on tolerability and degree of efficacy observed. Daily dosage above 60 mg is not recommended. When in the judgement of the clinician a lower initial dose is appropriate, patients may begin treatment with Ritalin LA 10 mg.)|quote=值左起第18位存在換行符 (帮助); 请检查|access-date=, |date=中的日期值 (帮助)
^
Label of Ritalin LA. DailyMed.com. Novartis. Mid 2015 [January, 2017.].Initial Treatment
参数
The recommended starting dose of Ritalin LA is 20 mg once daily. Dosage may be adjusted in weekly 10 mg increments to a maximum of 60 mg/day taken once daily in the morning, depending on tolerability and degree of efficacy observed. Daily dosage above 60 mg is not recommended. When in the judgement of the clinician a lower initial dose is appropriate, patients may begin treatment with Ritalin LA 10 mg.)|quote=值左起第18位存在換行符 (帮助); 请检查|access-date=, |date=中的日期值 (帮助)
^ Label of Concerta. DailyMed.gov. Jassen Cilag. 2013 [January, 2017.].1 INDICATIONS AND USAGE
参数
CONCERTA® is indicated for the treatment of Attention Deficit Hyperactivity Disorder (ADHD) in children 6 years of age and older, adolescents, and adults up to the age of 65 [see CLINICAL STUDIES (14)].
A diagnosis of Attention Deficit Hyperactivity Disorder (ADHD; DSM-IV) implies the presence of hyperactive-impulsive or inattentive symptoms that caused impairment and were present before age 7 years. The symptoms must cause clinically significant impairment, e.g., in social, academic, or occupational functioning, and be present in two or more settings, e.g., school (or work) and at home. The symptoms must not be better accounted for by another mental disorder. For the Inattentive Type, at least six of the following symptoms must have persisted for at least 6 months: lack of attention to details/careless mistakes; lack of sustained attention; poor listener; failure to follow through on tasks; poor organization; avoids tasks requiring sustained mental effort; loses things; easily distracted; forgetful. For the Hyperactive-Impulsive Type, at least six of the following symptoms must have persisted for at least 6 months: fidgeting/squirming; leaving seat; inappropriate running/climbing; difficulty with quiet activities; "on the go;" excessive talking; blurting answers; can't wait turn; intrusive. The Combined Type requires both inattentive and hyperactive-impulsive criteria to be met.|quote=值左起第27位存在換行符 (帮助); 请检查|access-date=中的日期值 (帮助)
^
Label of Concerta. DailyMed.gov. Jassen Cilag. 2013 [January, 2017.].14.2 Adolescents
参数
In a randomized, double-blind, multicenter, placebo-controlled trial (Study 4) involving 177 patients, CONCERTA® was demonstrated to be effective in the treatment of ADHD in adolescents aged 13 to 18 years at doses up to 72 mg/day (1.4 mg/kg/day). Of 220 patients who entered an open 4-week titration phase, 177 were titrated to an individualized dose (maximum of 72 mg/day) based on meeting specific improvement criteria on the ADHD Rating Scale and the Global Assessment of Effectiveness with acceptable tolerability. Patients who met these criteria were then randomized to receive either their individualized dose of CONCERTA® (18 – 72 mg/day, n=87) or placebo (n=90) during a two-week double-blind phase. At the end of this phase, mean scores for the investigator rating on the ADHD Rating Scale demonstrated that CONCERTA® was statistically significantly superior to placebo.|quote=值左起第17位存在換行符 (帮助); 请检查|access-date=中的日期值 (帮助)
^
Label of Concerta. DailyMed.gov. Jassen Cilag. 2013 [January, 2017.].14.2 Adolescents
参数
14.3 Adults
Two double-blind, placebo-controlled studies were conducted in 627 adults aged 18 to 65 years. The controlled studies compared CONCERTA® administered once daily and placebo in a multicenter, parallel-group, 7-week dose-titration study (Study 5) (36 to 108 mg/day) and in a multicenter, parallel-group, 5-week, fixed-dose study (Study 6) (18, 36, and 72 mg/day).
Study 5 demonstrated the effectiveness of CONCERTA® in the treatment of ADHD in adults aged 18 to 65 years at doses from 36 mg/day to 108 mg/day based on the change from baseline to final study visit on the Adult ADHD Investigator Rating Scale (AISRS). Of 226 patients who entered the 7-week trial, 110 were randomized to CONCERTA® and 116 were randomized to placebo. Treatment was initiated at 36 mg/day and patients continued with incremental increases of 18 mg/day (36 to 108 mg/day) based on meeting specific improvement criteria with acceptable tolerability. At the final study visit, mean change scores (LS Mean, SEM) for the investigator rating on the AISRS demonstrated that CONCERTA® was statistically significantly superior to placebo.
Study 6 was a multicenter, double-blind, randomized, placebo-controlled, parallel-group, dose-response study (5-week duration) with 3 fixed-dose groups (18, 36, and 72 mg). Patients were randomized to receive CONCERTA® administered at doses of 18 mg (n=101), 36 mg (n=102), 72 mg/day (n=102), or placebo (n=96). All three doses of CONCERTA® were statistically significantly more effective than placebo in improving CAARS (Conners' Adult ADHD Rating Scale) total scores at double-blind end point in adult subjects with ADHD.|quote=值左起第17位存在換行符 (帮助); 请检查|access-date=中的日期值 (帮助)
^
Label of Ritalin LA. DailyMed.com. Novartis. Mid 2015 [January, 2017.].Maintenance/Extended TreatmentThere is no body of evidence available from controlled trials to indicate how long the patient with ADHD should be treated with Ritalin LA. It is generally agreed, however, that pharmacological treatment of ADHD may be needed for extended periods. Nevertheless, the physician who elects to use Ritalin LA for extended periods in patients with ADHD should periodically re-evaluate the long-term usefulness of the drug for the individual patient with trials off medication to assess the patient’s functioning without pharmacotherapy. Improvement may be sustained when the drug is either temporarily or permanently discontinued.)
请检查|access-date=, |date=中的日期值 (帮助)
^ 管制藥品分級及品項
^ 国家食品药品监督管理局. 精神药品品种目录(2007年版). 医药网. 2007-10-31 [2013-02-04].
^ 处方管理办法(原卫生部令第53号). 中国政府网. 2007-03-13.
| ||||||||||||||||||||||||||||||||||||||||
| ||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||
| |||||||||||||||||
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||


